Introduction
The Canadian advisory board on dentin hypersensitivity ( 2003 ) defined Dentin hypersensitivity (Tooth sensitivity) as “a short, sharp pain arising from exposed dentin in response to stimuli typically thermal, evaporative, tactile, osmotic or chemical and which cannot be ascribed to any other form of dental defect or disease.” It has been described as the “common cold of dentistry” by some and
“toothbrush disease” by others when it occurs in the presence of gingival recession (Pashley et al. 2008 ).
Prevalence and Distribution
The condition is mostly prevalent among the young population in the 3rd and 4th decades. The prevalence may shift in the future to a younger age group because of the increase in acidic food/drink intake and the influence of greater oral hygiene awareness and measures (Chabanski et al. 1997; Clayton et al. 2002 ). Various intraoral locations can be affected with Dentin hypersensitivity. Sites of predilection in descending order are canines and first premolars, incisors and second premolars, and molars (Dababneh et al. 1999 ). The buccal surfaces are mostly affected, followed by labial, occlusal, distal, and lingual. Incisal and palatal surfaces are the least affected (Splieth and Tachou 2012; Amarasena et al. 2011 ).
Mechanism
Brännström’s ( 1962, 1992 ) hydrodynamic theory of dentin sensitivity proposed that hydrodynamic
stimuli (hot or cold, tactile, evaporative or osmotic) caused sudden minute shifts of dentinal fluid that activate pulpal mechanoreceptors to cause sharp, well-localized tooth pain, thought to be due to A-delta sensory nerves (Narhi et al., 1992 ).
Causes and Predisposing Factors
The most important factor to be present for tooth sensitivity is the loss of tooth structure and the exposure of dentin to the oral cavity. The dentin may be exposed to the oral cavity by either the loss of enamel or cementum and overlying periodontal attachment apparatus or loss of both at the same time. Following the exposure, the patent dentinal tubules remain wide open and thus are predisposed to any stimulus, called the phase of “lesion initiation.” However, not all exposed dentin is sensitive (Rimondini et al. 1995 ).
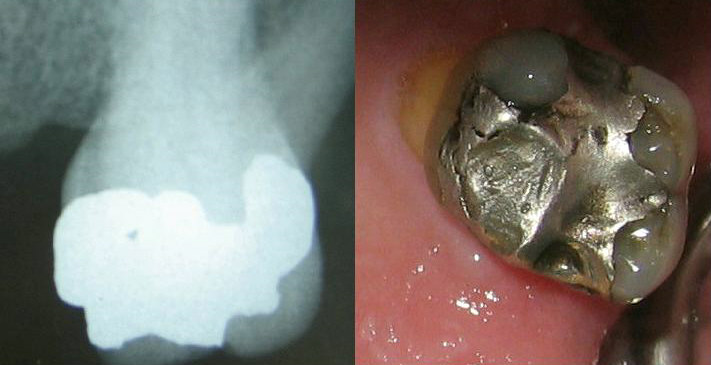
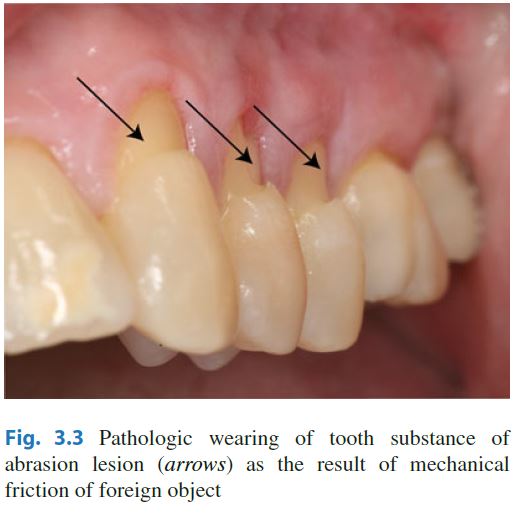
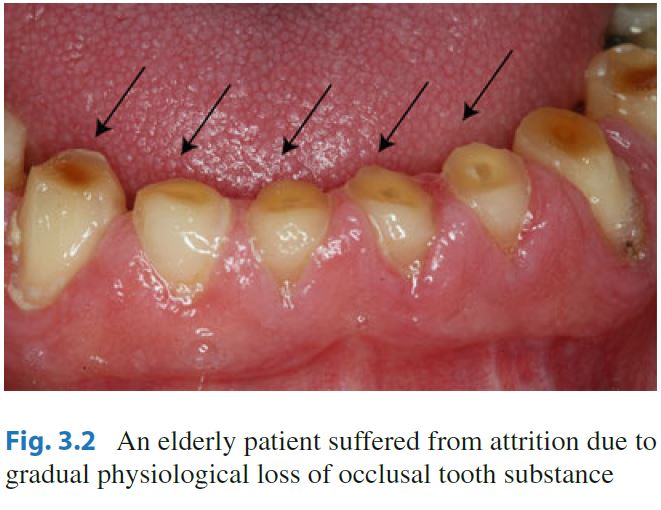
The loss of enamel may be either due to attrition, erosion, abrasion, abfraction or abrasion due to tooth brushing (most commonly cervical abrasion). Similarly, loss of cementum due to various causes and periodontal attachment loss may cause exposure of dentinal tubules. Some medical conditions like Bulimia Nervosa, Gastroesophageal reflux disease, Chronic alcoholism, Salivary hypofunction, etc. may also cause dentin hypersensitivity.
Diagnosis
Diagnosis of dentin hypersensitivity can be made by applying any of the mechanical, chemical, thermal or electrical stimuli. Electronic pulp testers (EPT), mechanical pressure stimulators, air jet stimulator, ethyl chloride, thermoelectric device, cold water testing, ice testing, etc. can be used for challenging the affected tooth.
Treatment
Two treatment approaches are mainly practiced in the treatment of dentin hypersensitivity. They are:
- Use of dentin blocking agents that occlude patent (open) tubules (fluoride, strontium salts, oxalate, calcium phosphate, restorative materials, etc.), and
- Nerve desensitization agents that reduce intradental nerve excitability (e.g. potassium ions, guanethidine) in order to prevent a response from intra dental nerves to the stimulus- evoked fluid movements within the dentin tubules
Application of these successfully tested products may either involve ‘in-office’ procedures by a clinician using a restorative approach (for example, restorative materials in the form of dentin bonding agents, glass ionomer cements (GIC), and periodontal surgical techniques) or by a clinician recommending an over-the-counter (OTC) approach (involving toothpastes, gels, mouthwashes).
Furthermore, the causative agent has to be identified and avoided as much as possible and the patient should be educated about the proper brushing technique to prevent mechanical abrasion due to toothbrushing in the future.
References:
1. Canadian Advisory Board on Dentin Hypersensitivity (2003) Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc 69(4):221–226
2. Pashley DH, Tay FR, Haywood VB, Collins MA, Drisko CL (2008) Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. Inside Dentistry 4(9 (Special Issue)):1–35
3. Chabanski MB, Gillam DG, Bulman JS, Newman HN (1997) Clinical evaluation of cervical dentine sensitivity in a population of patients referred to a specialist periodontology department: a pilot study. J Oral Rehabil 24(9):666–672
4. Clayton DR, McCarthy D, Gillam DG (2002) A study of the prevalence and distribution of dentine sensitivity in a population of 17-58-year-old serving personnel on an RAF base in the Midlands. J Oral Rehabil 29(1):14–23, 805 [pii]
5. Dababneh RH, Khouri AT, Addy M (1999) Dentine hypersensitivity – an enigma? A review of terminology, mechanisms, aetiology and management. Br Dent J 187(11):606–611; discussion 603. doi: 10.1038/sj.bdj.4800345a , 4800345a [pii]
6. Brännström M (1992) Etiology of dentin hypersensitivity. Proc Finn Dent Soc 88(Suppl 1):7–13
7. Brännström M (1962) The elicitation of pain in human dentine and pulp by chemical stimuli. Arch Oral Biol 7:59–62
8. Närhi M, Jyvasjarv E, Vitanen A, Huopaniemi T, Ngassapa D, Hirvonen T (1992) Role of intra dental A and C type nerve fibers in dental pain mechanisms. Proc Finn Dent Soc 8(Suppl 1):507–516
9. Dababneh RH, Khouri AT, Addy M (1999) Dentine hypersensitivity – an enigma? A review of terminology, mechanisms, aetiology and management. Br Dent J 187(11):606–611. doi: 10.1038/sj.bdj.4800345a ; discussion 603
10. Clinician’s Guide to the Diagnosis and Management of Tooth Sensitivity ; Sahar Taha, Brian H. Clarkson ISBN 978-3-642-45163-8 ISBN 978-3-642-45164-5 (eBook) DOI 10.1007/978-3-642-45164-5
11. Rimondini L, Baroni C, Carrassi A (1995) Ultrastructure of hypersensitive and non-sensitive dentine. A study on replica models. J Clin Periodontol 22(12):899–902
12. Ling TYY, Gillam DG (1996) The effectiveness of desensitizing agents for the treatment of cervical dentine sensitivity (CDS) – a review. Periodontal Abstr 44(1):5–12
13. Orchardson R, Gillam D (2006) Managing dentin hypersensitivity. J Am Dent Assoc 137(7):990–998