This is one of the most frequently faced questions by a dentist, "Doctor, How long will my dental restoration last?" In the competitive world of today, people are taken away by the fake promises and guarantees the corporations and manufacturer companies make and expect everything to have a guarantee. But, this question, in particular, is ridiculous because we cannot predict the health or disease of any person or how long will he last!
But, answering the question, the life of any dental restoration depends principally upon four factors:
- remaining tooth structure
- material with which the tooth is being restored
- clinical technique & expertise of the dentist i.e. how well the restoration is done
- post-restoration environmental challenges the tooth is subjected to
Let's see all these one by one.
i) Remaining tooth structure
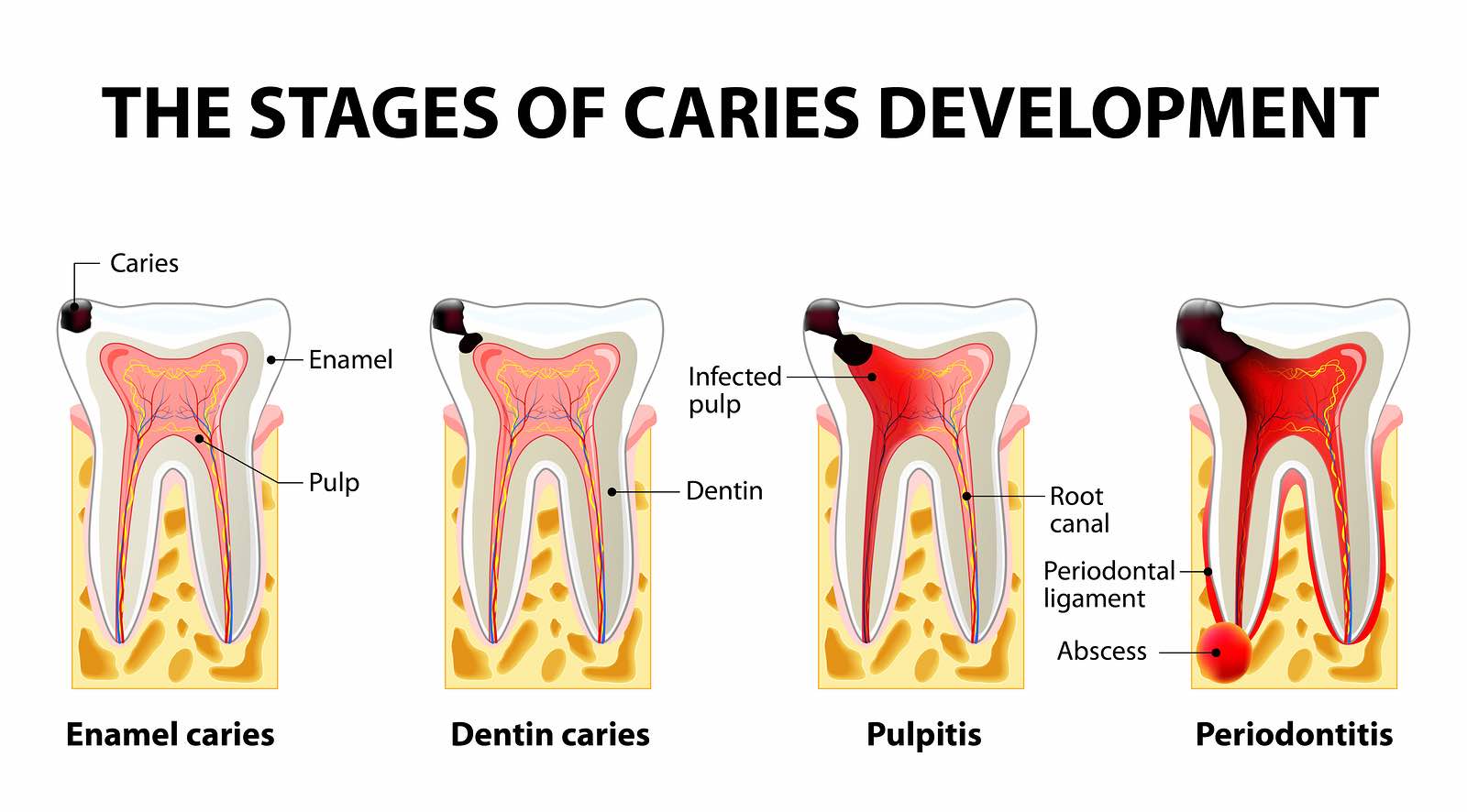
"A stitch in time saves nine." This age-old proverb can be well realized in dentistry. We can expect the dental restorations' cost to be cheaper, less time consuming and successful for a long time too if the treatment is done as early as possible. We cannot expect a tooth with cavity extending up to the cervical third of crown involving pulp with almost two-thirds of the crown lost already to have the same prognosis as that of the tooth with cavity extending only up to the enamel layer or superficial dentinal layer.
A restoration may fail due to several reasons:
No 1. - Restoration may fracture if its bulk is too small or its mechanical strength is too low.
No 2. - The tooth may fracture if most of the tooth structure is already lost or excessive occlusal force is applied on the restored tooth.
No. 3 - Failure at the tooth restoration junction: If there is no proper seal at the tooth restoration junction, the food materials, and bacteria can percolate through the breach into the tooth and can cause secondary caries.
Let's see the second factor determining the life of dental restoration.
ii) Material with which the tooth is being restored :
Three major dental restorative materials currently used in dentistry are:
- Glass ionomer cement
- Dental composite resins
- Amalgams (not used in many countries but still used in some due to the environmental hazard of mercury)
Different types of glass ionomer cement according to their use are available. Glass ionomers are used mostly in the deciduous teeth of children but they can be used adults too and latest GICs with improved properties have been reported to last about 3-5 years too.
Regarding dental composite resins and amalgams, they have similar strength and longevity provided that, the restoration is done meticulously in ideal conditions.
A rule of thumb for clinical service of restoration is that occlusal restorations are stressed an average of one million times per year. And, typically material fails in the range of 10-100 million cycle range during laboratory testing.
Also, different products from different manufacturers have different mechanical properties. You cannot expect a composite resin from some unknown manufacturer in China to work equally well as that from an internationally renowned brand.
The third factor determining the longevity of restoration is the clinical technique and expertise.
iii) How well the dentist has restored the tooth?
Just because the dentist is old and experienced doesn't mean that he will do the restoration well. A dentist who can do well, may not do his best at all times if he is inattentive or is in a hurry. Improper isolation of tooth and contamination by saliva during the procedure also might have compromised the strength.
And the last and most important factor for the longevity of dental restorations is:
iv) Post-restoration environmental challenges the tooth is subject to
How long would your house last if it were subjected to hot sweet coffee and immediately to freezing cold ice cream? How long would it last if it were struck for about 5000 times daily? What if it is subjected to acidic pH as low as 3 and to alkaline pH as high as 11 within a few minutes? That is what our dental restoration has to sustain. We eat and drink acidic and alkaline foods, hard and soft foods, cold and hot foods, every sort of food without any consideration. How long will it be before the material fatigue occurs in the restoration and breaks down?
By now, you might have understood what I mean to say. But it is a safe bet to say that dental restorations will last about an average of 6-8 years if all the above factors are considered. However, there are cases of restoration failures the very next day as well as some amalgam restorations about 30 years old.
How long has your restoration lasted? What was the material? Please Comment Below for record purpose. Feedback and Suggestions for the article are heartily welcome.