This post contains 33 sorted diagrams of histopathological pictures of pathologies related to oral and maxillofacial regions. From benign to malignant neoplasms of oral cavity, salivary gland tumors, cyst and tumors of jaws and oral cavity, to lesions affecting nerves and muscles and soft tissues, it contains all you need to have a good command in oral pathology.
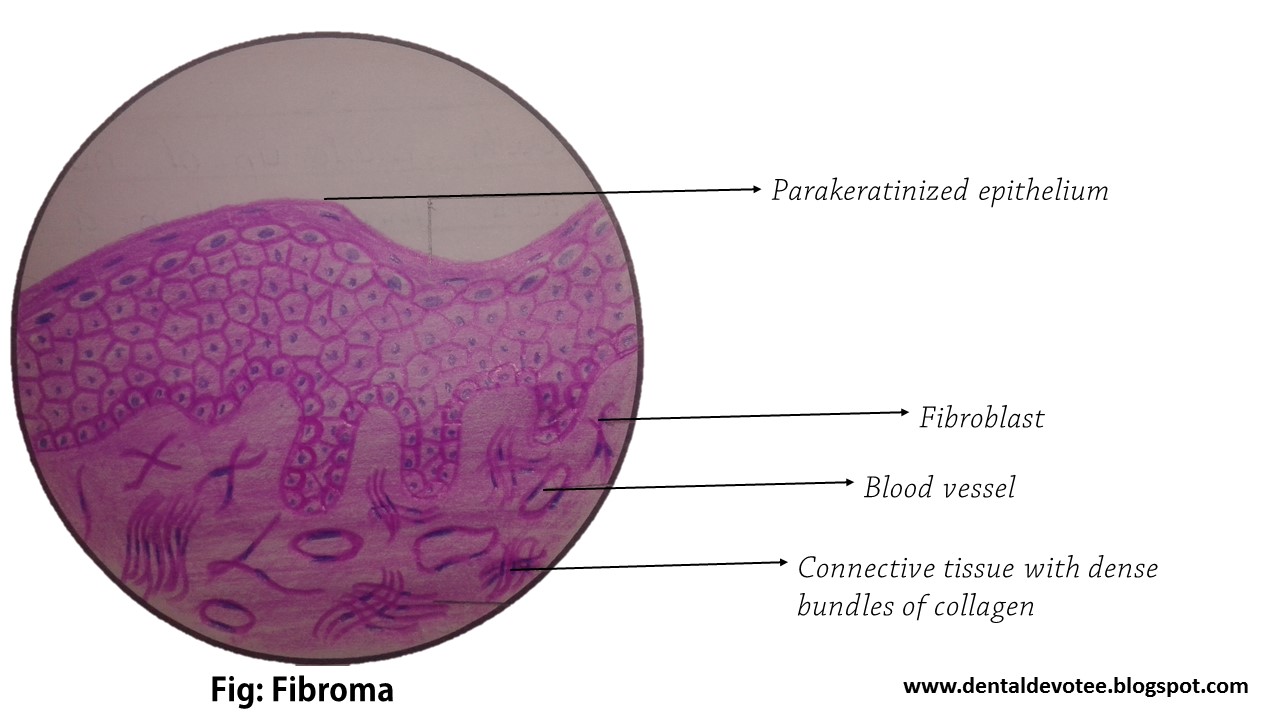
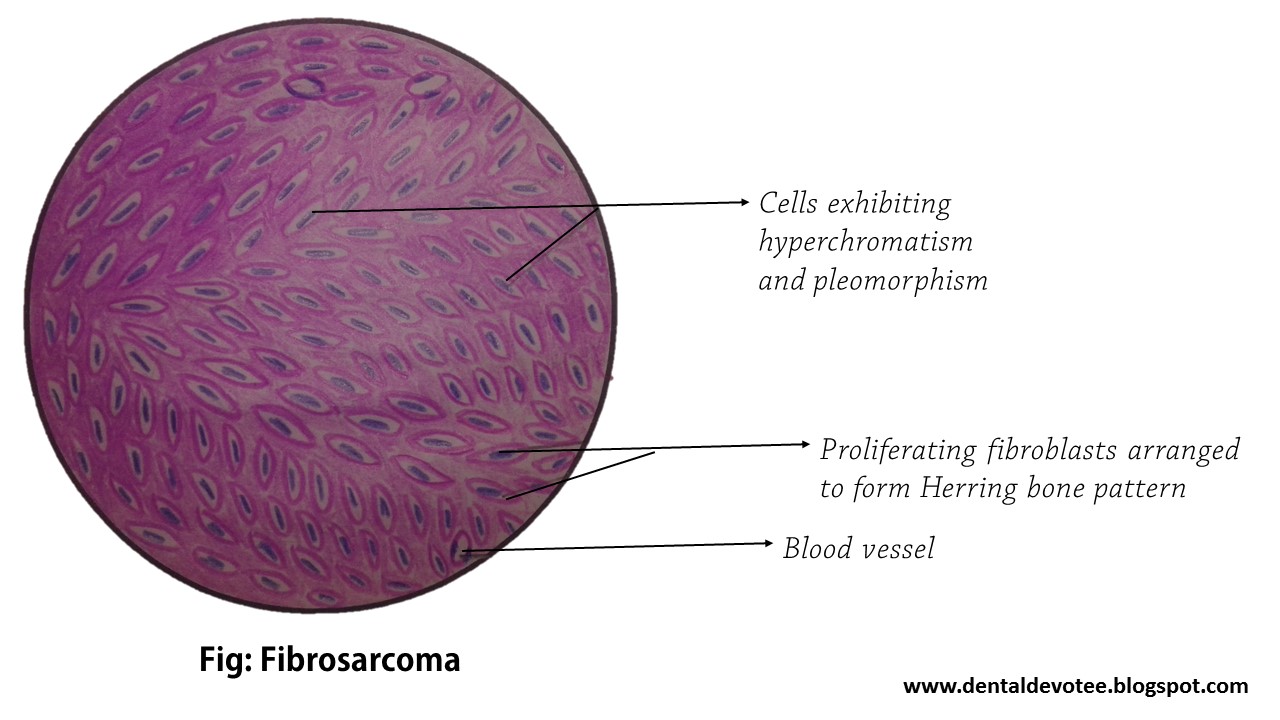
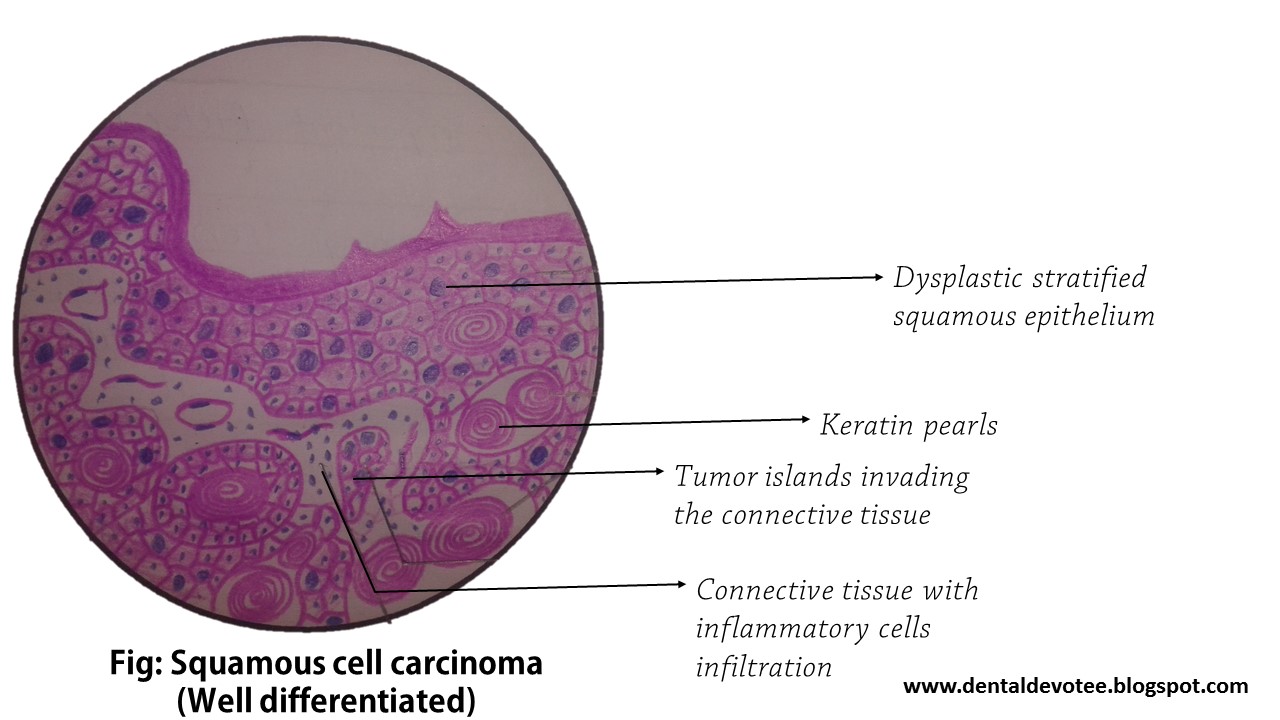
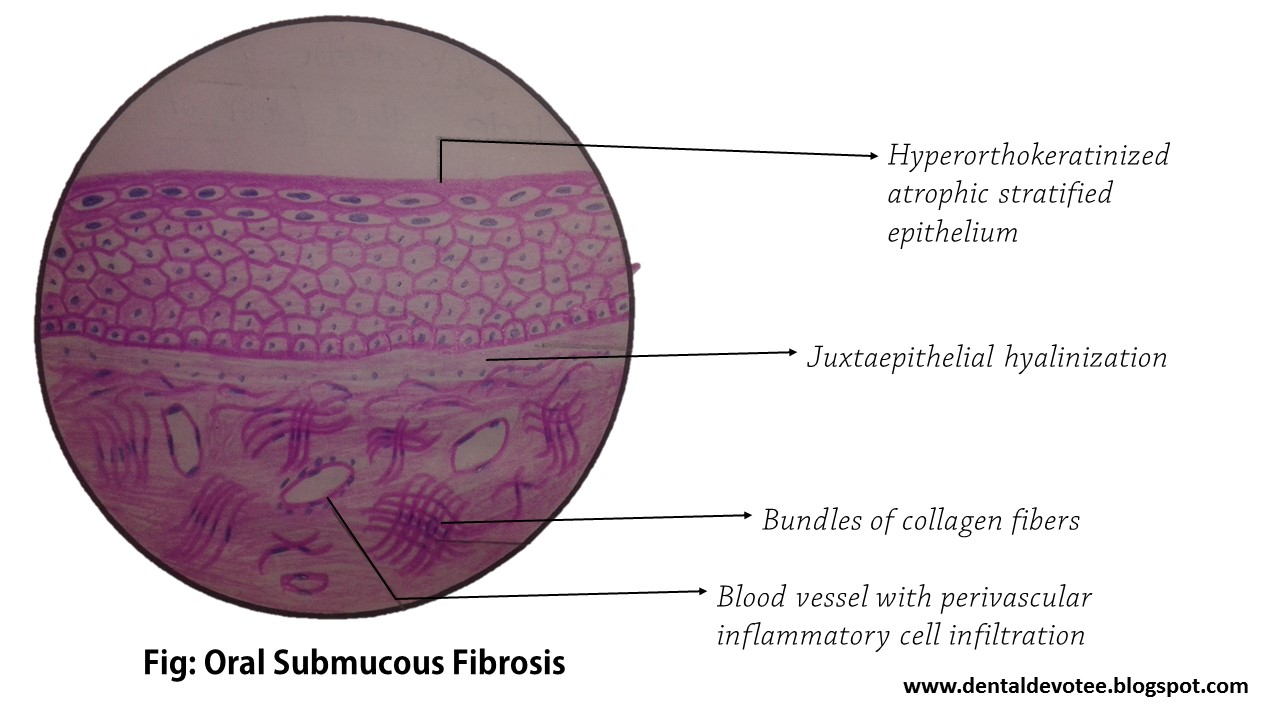
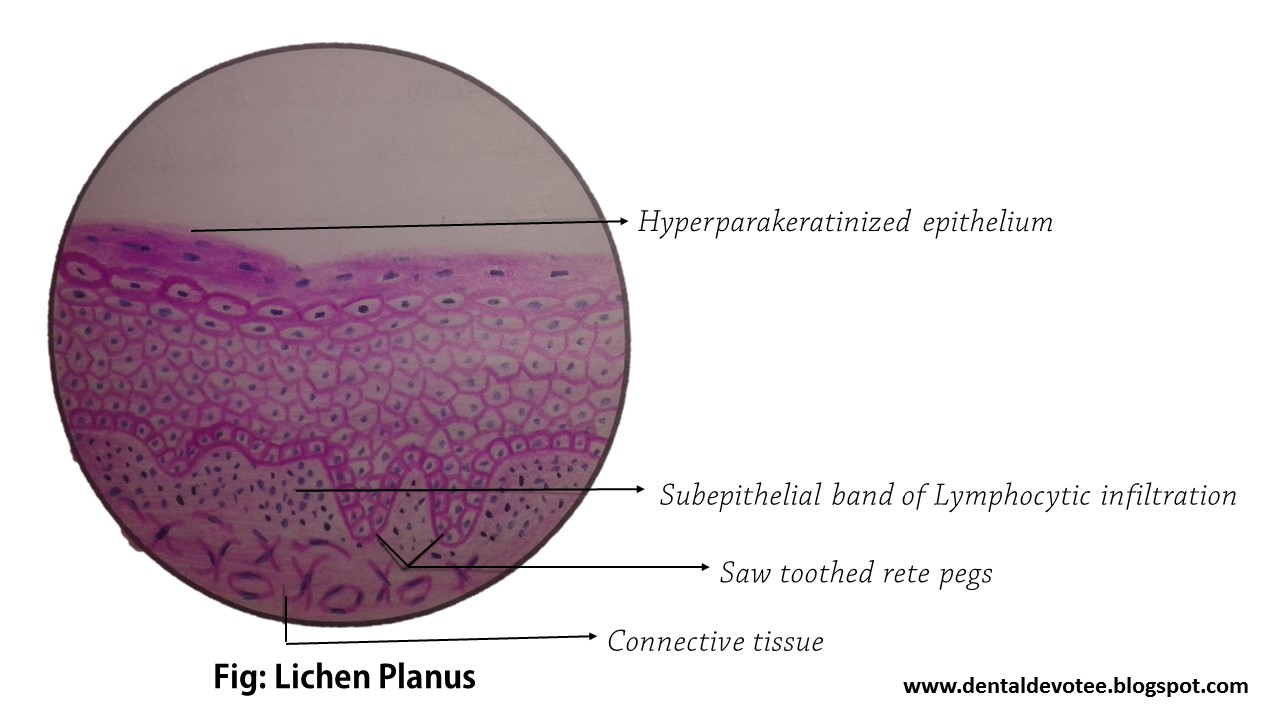
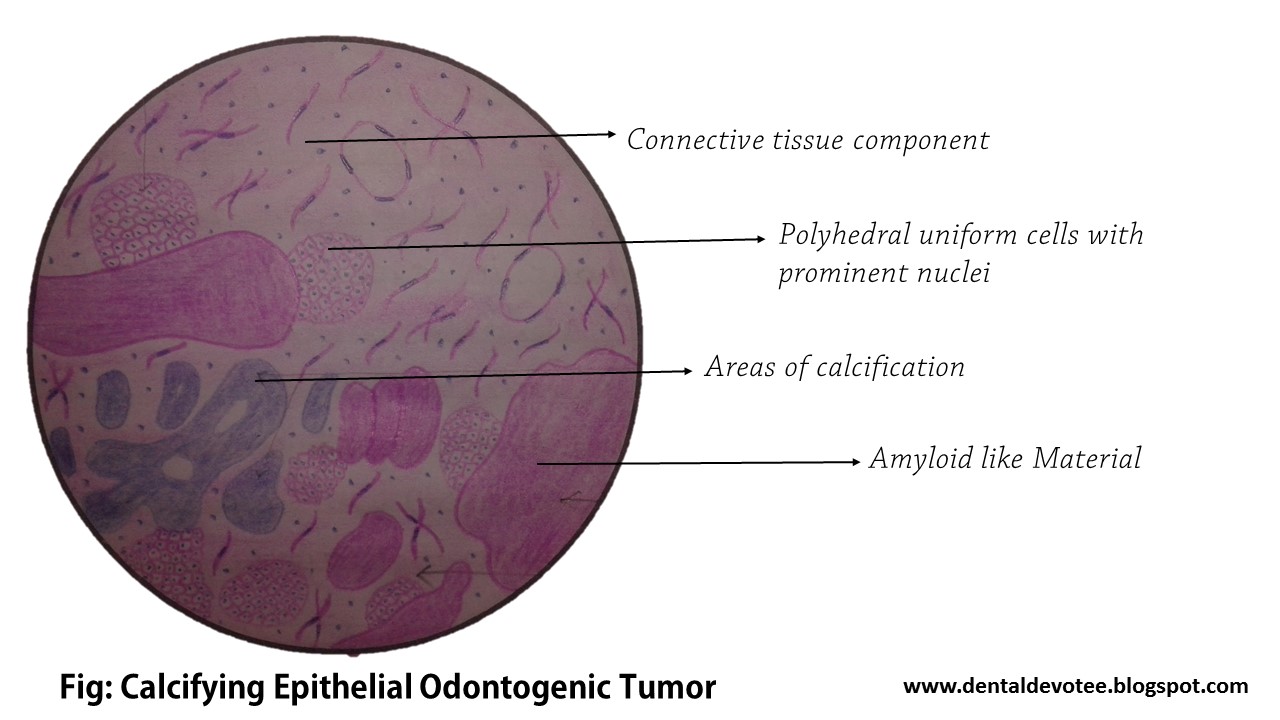
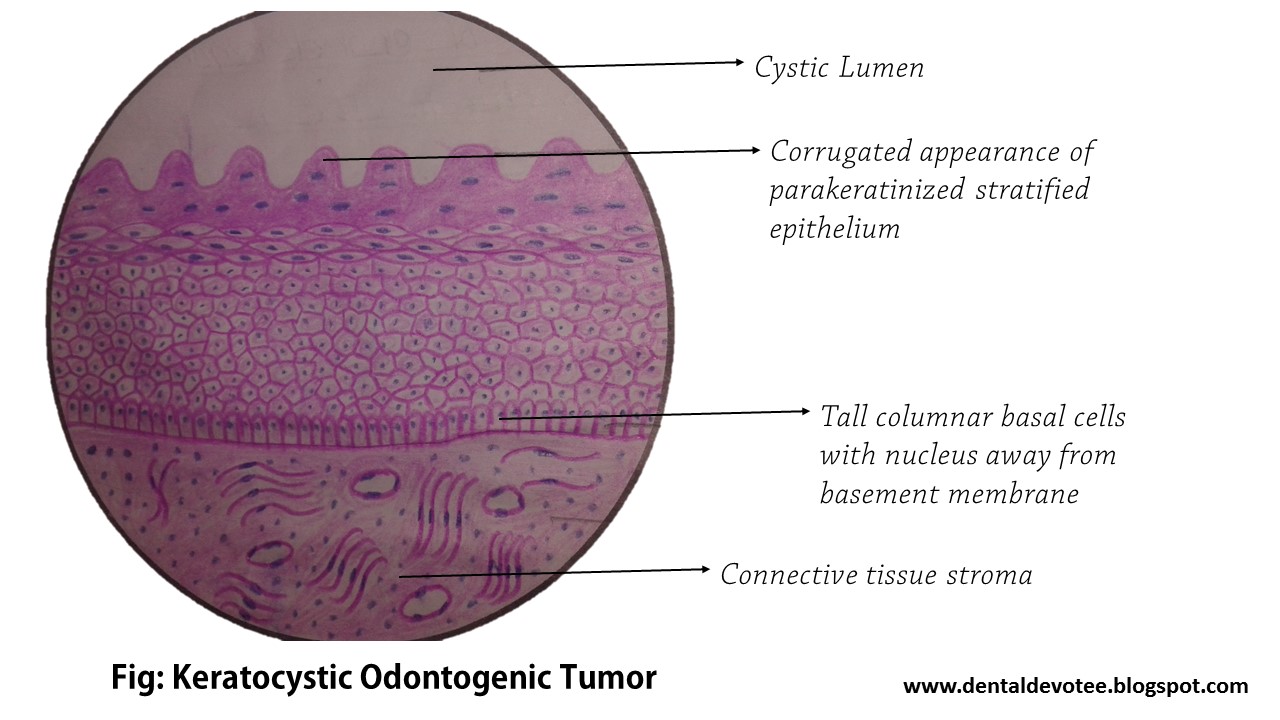
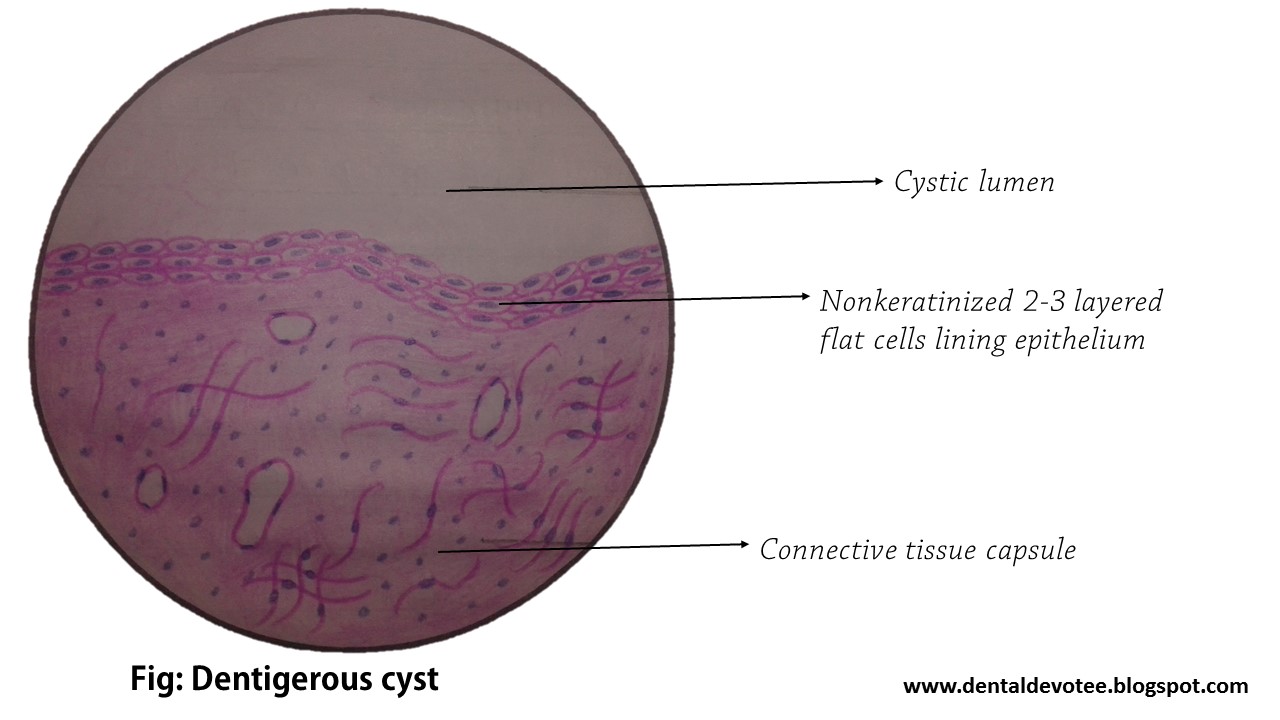
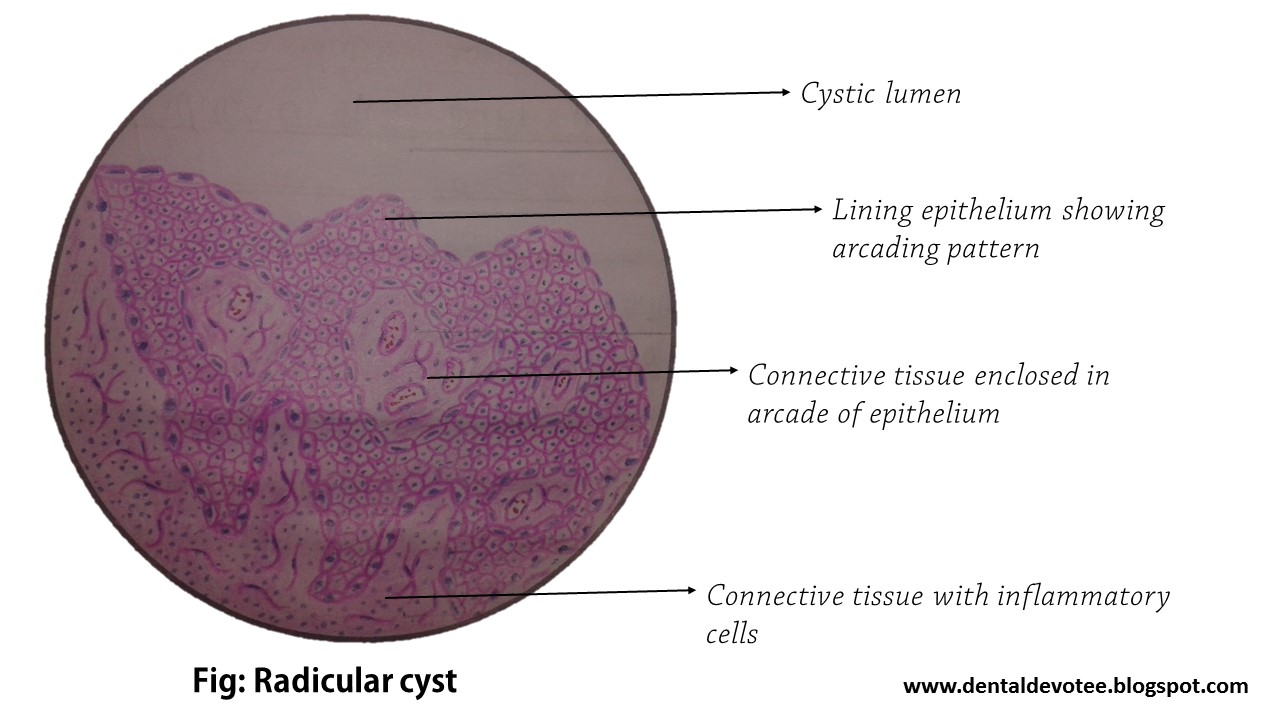
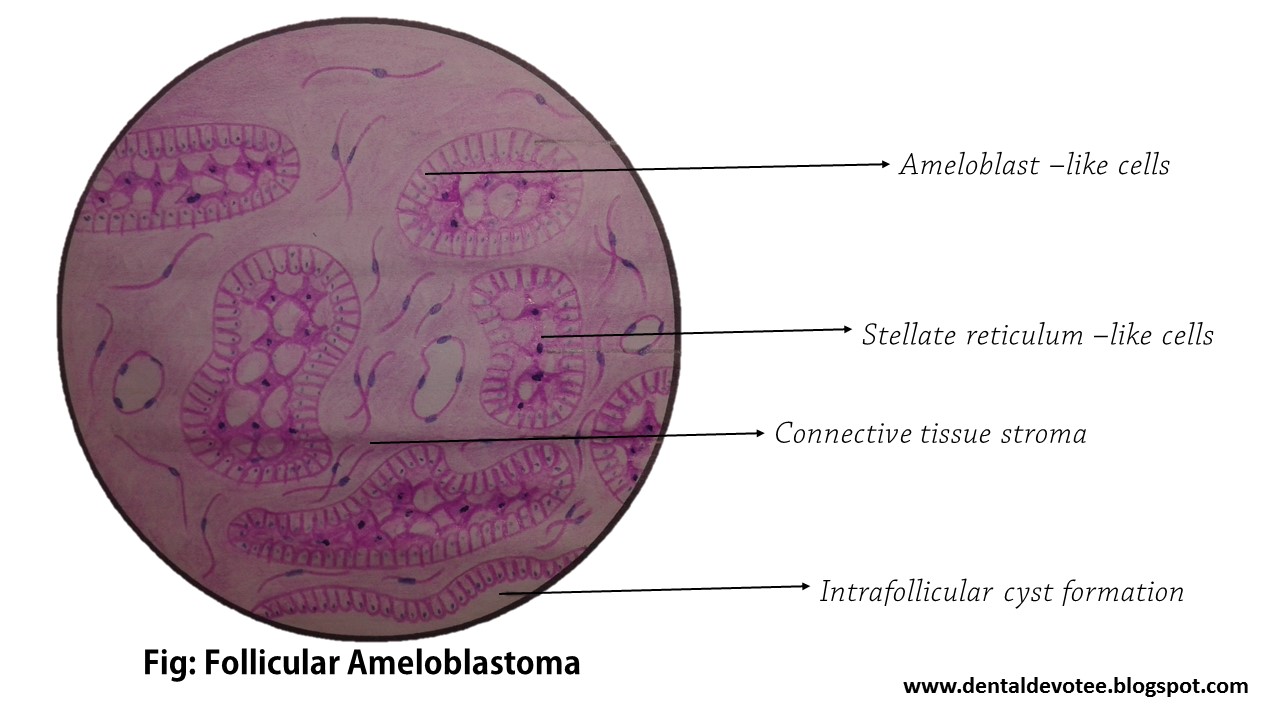
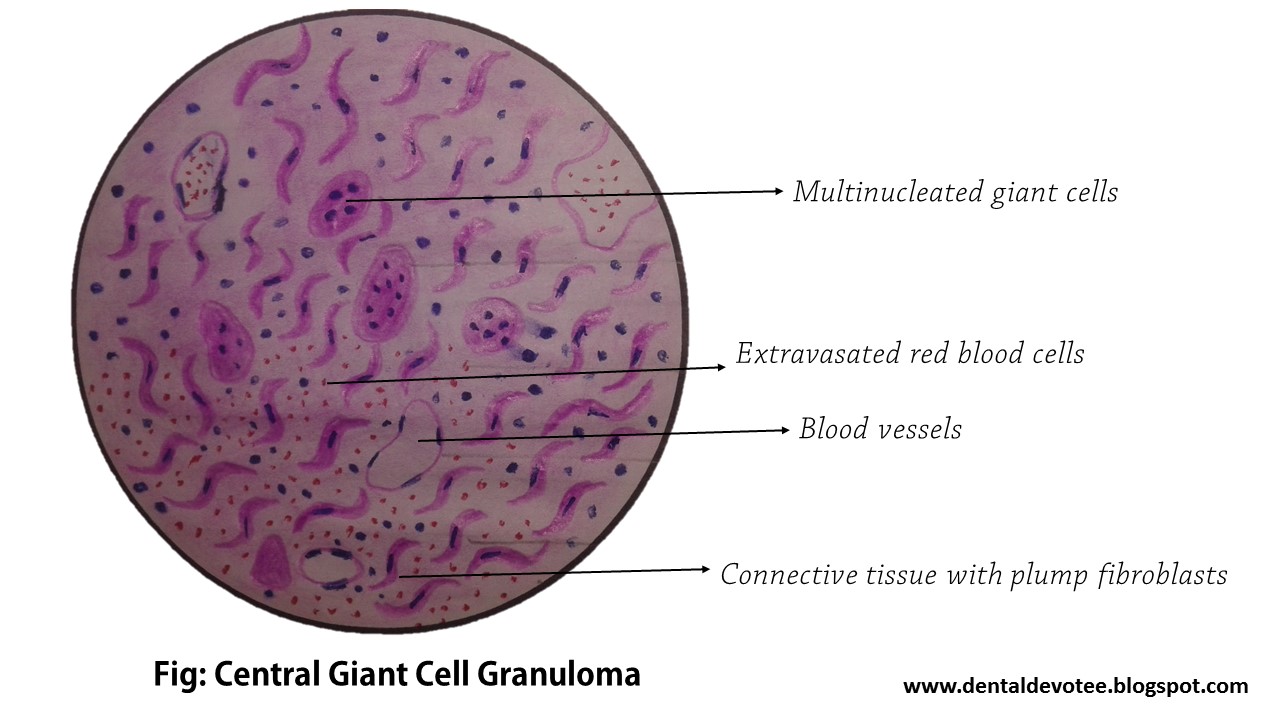
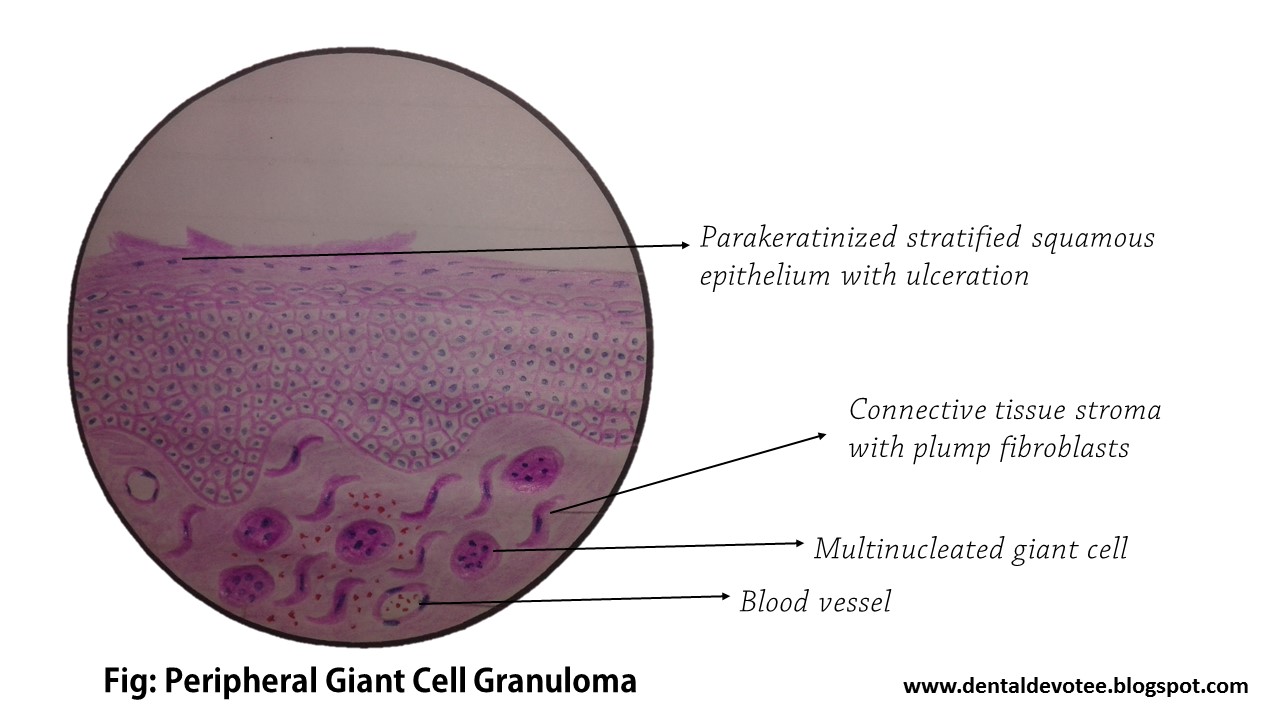
These diagrams were drawn with Hematoxylin and Eosin colored Pencils by Raman Dhungel during his Bachelor of Dental Surgery course on third year at B.P. Koirala Institute of Health Sciences, BPKIHS Dharan. The slides included in this video are: Fibroma, FIbrosarcoma, Papilloma, Verrucous carcinoma, Mild dysplasia, Carcinoma in situ, Squamous cell carcinoma (well differentiated), Neurilemmoma, Neurofibroma, Oral submucous fibrosis, cavernous hemangioma, Lipoma, Lichen planus, malignant melanoma, osteosarcoma, pleomorphic adenoma, warthin's tumor, Adenoid cystic carcinoma, Mucoepidermoid carcinoma, Calcifying epithelial odontogenic tumor, Adenomatoid odontogenic tumor, Keratocystic odontogenic tumor, Dentigerous cyst, Radicular cyst, Plexiform ameloblastoma, Follicular ameloblastoma, Central giant cell granuloma, Peripheral giant cell granuloma, Fibrous dysplasia, Paget's disease of bone, Pemphigus, Pemphigoid (Bullous pemphigoid), and pyogenic granuloma.
Much time and effort was needed to produce this post. We would be gratified to know that if this postbecomes of some help to you. Please share with your friends and students too.